What did we select?
The National Institutes of Health (NIH)
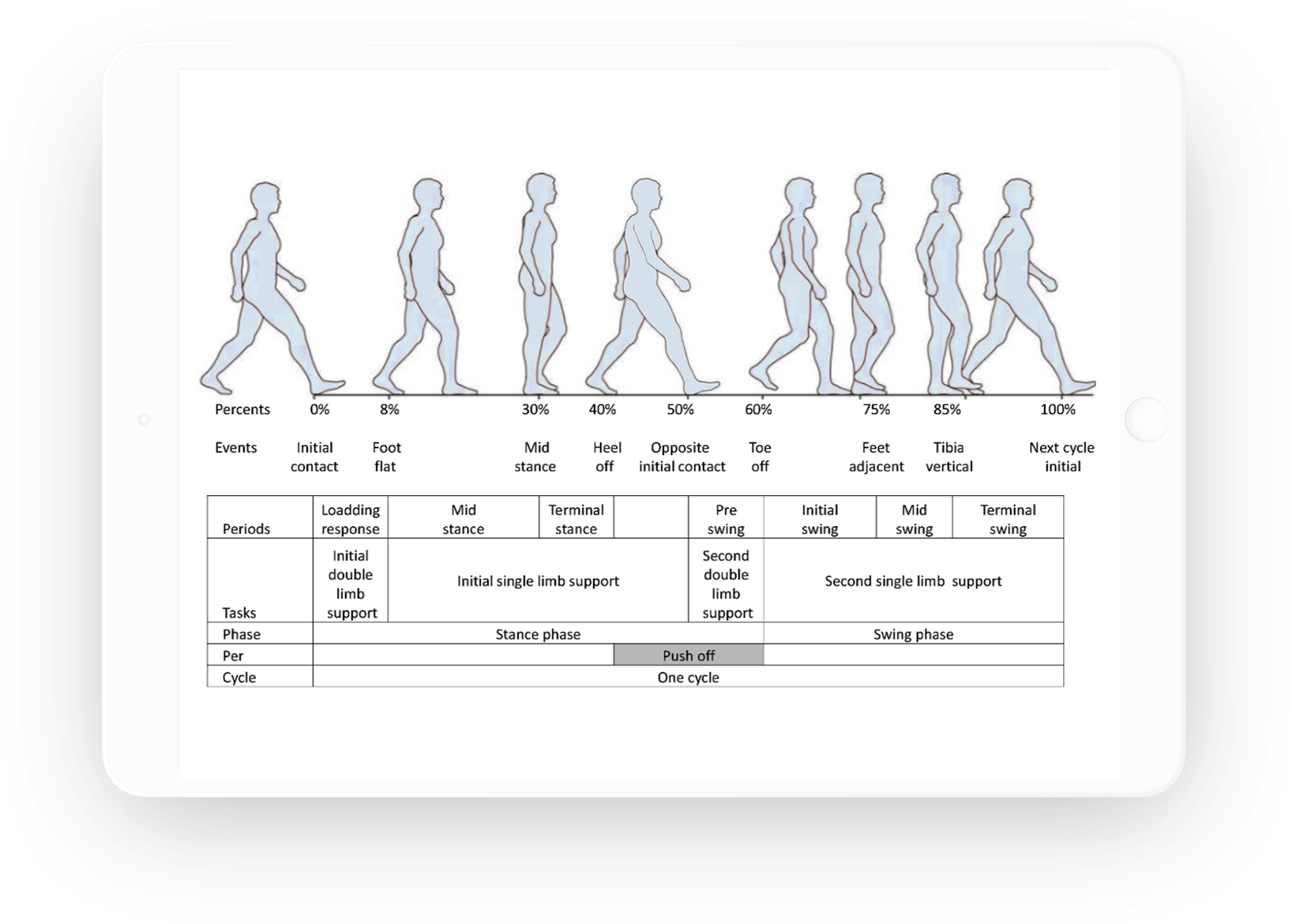
4-Meter Gait Test is a gait test commonly used to assess
walking speed over a short distance. Gait
involves dynamic postural control, where the
individual changes their base of support
throughout the movement. Gait slowing
effects have been shown to be remarkably
reliable and durable over time (Parker et
al., 2006).
The 4-meter gait test has proven to be
remarkably reliable, consistently yields
some of the highest reliability
coefficients, with inter- class correlation
coefficients (ICC) values of .96 to .98 for
adults (Peters et al., 2013) and ICCs of .81
for adolescents (Alsalaheen, 2014).
Why we selected it
The research has demonstrated the NIH
4-meter test’s strong characteristics:
Test-Retest Reliability:
0.96 to 0.98 for adults (Peters et al.,
2013); 0.81 for adolescents (Alsalaheen,
2014)
Normative Data:
stratified by age and gender (National
Institutes of Health)
-
Age range: 5-85 years from NIH Toolbox
(Kallen et al., 2012)
- Gender: Male and female
No documented ceiling or practice effects
with repeat testing.
What did we select?
The Balance Error Scoring System (BESS) is an assessment to measure static balance
and postural control. Postural control is an
individual’s amount of sway, with greater
neuromotor control associated with less
postural sway.
The full BESS has been shown to have
reliability ranging from moderate to good
(Chang et al., 2014), with reliability
coefficients of .7 achieved in a sample of
children and adolescents, when using
separate norms for men and women (Mcleod et
al., 2006; note: test–retest values of more
than .90 can be obtained when taking the
average of multiple BESS administrations in
one day; Broglio et al., 2009.)
The computerized BESS, which automates and
facilitates the delivery and timing of the
full BESS, was more recently developed to
provide a more objective and quantitative
method of assessing balance errors.
Comparisons of the computerized BESS to
standard scoring procedures have shown that
computerized BESS scoring is more sensitive
in its measurements of performance and
postural stability than scores calculated
from traditional motion capture data alone
(Alberts et al., 2014). Additionally,
inter-rater reliability between computerized
and standard human-calculated BESS scores
have been found to range from fair to
excellent (0.44-0.99) across the six main
stances (Caccese & Kaminski, 2014; cf.
Houston et al., 2019). With respect to
validity, the computerized scores are
generally equivalent to human-rated scores
across balance conditions (Glass et al.,
2019).
Why we selected it
The following research has demonstrated
strong characteristics of the BESS:
Test-Retest Reliability:
0.70-.90 in children and adults (e.g.,
Mcleod et al., 2006)
Normative Data:
stratified by age and gender (e.g.,
Iverson & Koehle, 2013).
-
Age range: 5 to 23 stratified by age and
gender, age 24+ stratified by age (e.g.,
Iverson & Koehle, 2013).
- Gender: Male and female
No documented practice or ceiling effects.